COVID 19 Pandemic Highlights Health Disparities and the Need for Trial Diversity

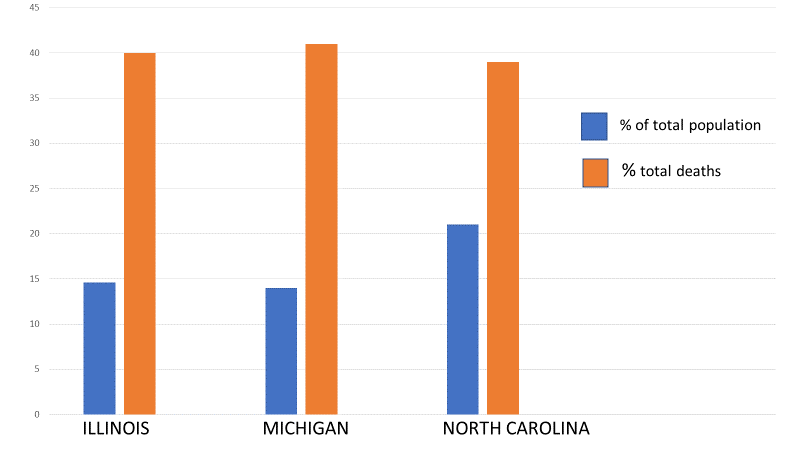
The first case in the United States of the virus (SARS-CoV-2) that caused coronavirus disease 2019 (COVID-19) was identified in Washington State on January 20, 2020.1 In April 2020, it appears that people across all states, Washington D.C., and four U.S. territories, have tested positive for the virus. As of April 12, 2020, the number of total cases in the United States is 525,704 and the number of total deaths is 20,486.2 As some states have begun to release mortality rates based on race and ethnicity, reports are emerging that COVID-19 is disproportionately impacting African Americans (see Figure 1).
Figure 1. Percentage of COVID-19-associated deaths for African Americans in Illinois, Michigan, and North Carolina by race/ethnicity
Higher hospitalizations rates are associated with comorbid health conditions. The Centers for Disease Control and Prevention (CDC) is conducting population-based surveillance study for hospitalizations associated with COVID-19. Data from the network (COVID-19 – Associated Hospitalization Surveillance Network [COVID-NET]) documented that hospitalizations increased among select groups: persons aged 65 years or older, men, and those with comorbid health conditions such as chronic lung disease, cardiovascular disease, obesity, hypertension, and diabetes mellitus.3
There is a higher prevalence of traditional cardiovascular risk factors in African Americans (e.g., hypertension, diabetes mellitus),4 and although age adjusted death rates for heart disease between 1999 to 2017 decreased for all racial/ethnic groups, non-Hispanic blacks were more than twice as likely as non-Hispanic Asian or Pacific Islanders to die of heart disease based on data from 1999–2017.5 This information gives us a better understanding of why African Americans are more likely to be hospitalized for COVID-19 disease.
Differences in health conditions are influenced by our social and physical environment. In addition to health behaviors and family history, our health is closely linked to where we live, learn, work and play (i.e., social determinants of health). Social determinants of health have a significant influence on our quality of life. For example, children who live in federally assisted housing are at higher risk for lead exposure which can have serious consequences for their health (e.g., behavioral disorders, neurologic problems and even death).6 Emerging research also supports the detrimental role of discrimination on health, at both the interpersonal (e.g., stressful life experiences adversely affecting health) and the institutional level (e.g., contribution of residential segregation to racial inequities in health).7 In addition to increased risk of chronic diseases, certain communities have the additional burden of social and physical factors that negatively impact their health.
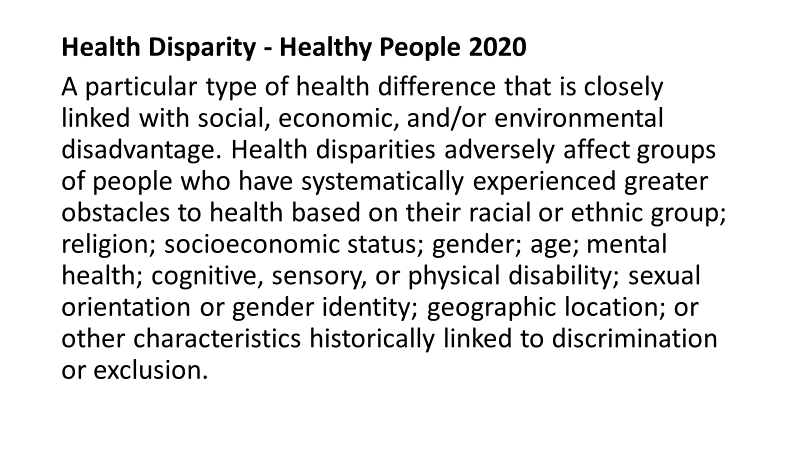
The coronavirus pandemic brings our focus back to health disparities. Emerging data of disproportionate rates of COVID-19 disease and death affecting African Americans is an “eye-opening” reminder that brings renewed awareness to overall disparities in health (see Figure 2 for Healthy People 2020 definition). The coronavirus pandemic provides a wakeup call that we still have work to do when comes to addressing the healthcare needs of all our communities. As a nation, it is in all our collective best interest to ensure good health for everyone. In doing so, we must value everyone equally with focused and ongoing societal efforts to address avoidable inequalities and historical and contemporary injustices.
Figure 2. Healthy People 2020 definition of Health Disparities 8
The public health approach must be to define and measure the problem to adequately address the disparity. On March 27, 2020, Sen. Elizabeth Warren and Rep. Ayanna Pressley, of Massachusetts, sent a letter to the Secretary of Health and Human Services (HHS) Alex Azar requesting that the Federal Government improve efforts to collect and publicly report on the racial and ethnic demographic information of patients with COVID-19.9 In the letter, they noted that “without demographic data on the race and ethnicity of patients being tested, the rate of positive test results, and outcomes for those with COVID-19, it will be impossible for practitioners and policy makers to address disparities in health outcomes and inequities in access to testing and treatment as they emerge. This lack of information will exacerbate existing health disparities and result in the loss of lives in vulnerable communities.” This request harkens back to about 35 years ago, when the Secretary of HHS, Margaret Heckler, formed a task force to examine factors that contributed to disparities in health. The subsequent Heckler Report documented health disparities and made a number of recommendations, one of which noted that “reliable data are central to measuring progress in public health, and are the key to assessing the current health status of the Nation and measuring health status trends.” 10
Moving forward with an eye on diversity and inclusion. As we work to discover a treatment for COVID-19 disease, I hope that we can implement the following: (1) we must expand reporting of demographic statewide testing data, (2) we must ensure we are providing adequate resources to test individuals in communities that are being disproportionately impacted by the pandemic, and (3) we must encourage sponsors to actively seek diverse representation in clinical trials, to ensure we have the best understanding of how different groups might respond to new treatments. Emerging data supports the disproportionate impact of COVID-19 disease on the African American community. It would be a monumental health risk to ignore this data, and this community, as we search for a solution.
Regina James, M.D.
Senior Vice President & Chief Medical Officer
2M Clinical
www.2Mclinical.com
References
- Omer, S. B., Malani, P., & del Rio, C. (2010, April 6). The COVID-19 pandemic in the US: A clinical update. Journal of American Medical Association (online). doi:10.1001/jama.2020.5788
- Centers for Disease Control and Prevention. (2020, April 14). Cases in U.S. https://cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html
- Centers for Disease Control and Prevention. (2020, April 4). A weekly summary of U.S. COVID-19 hospitalization data. https://gis.cdc.gov/grasp/COVIDNet/COVID19_3.html
- Carnethon, M. R., Pu, J., Howard, G., Albert, M. A., Anderson, C. A. M., Bertoni, A. G., . . . Yancy, C. W. (2017, November 21). Cardiovascular health in African Americans: a scientific statement from the American Heart Association. AHA Journals 136(21): e393–e423. Prepared on behalf of the American Heart Association Council on Epidemiology and Prevention; Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; Council on Functional Genomics and Translational Biology; and Stroke Council. doi: 10.1161/CIR.0000000000000534.
- Centers for Disease Control and Prevention, National Center for Health Statistics. (2019, October 30). Health, United States.https://www.cdc.gov/nchs/hus/index.htm?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fnchs%2Fhus.htm
- Pell, M. B., & Schneyer, J. (2016, December 19). The thousands of U.S. locales where lead poisoning is worse than in Flint. https://www.reuters.com/investigates/special-report/usa-lead-testing/
- VanDyke, M. E., Baumhofer, N. K., Slopen, N., Mujahid, M. S., Clark, C. R., Williams, D. R., & Lewis, T. T. (2020, April). Pervasive discrimination and allostatic load in African American and White adults. Psychosomatic Medicine 82(3): 316–323. doi: 10.1097/PSY.0000000000000788
- Office of Disease Prevention and Health Promotion. (2020, April 14). Foundation Health Measures Archive: Disparities. https://www.healthypeople.gov/2020/about/foundation-health-measures/Disparities
- Warren, E., Pressley, A., Kelly, R. L., Harris, K. D., & Booker, C. A. (2020, March 27). Letter from the U.S. Congress to the Honorable Alex M. Azar, Secretary of the U.S. Department of Health and Human Services. https://www.warren.senate.gov/imo/media/doc/2020.03.27%20Letter%20to%20HHS%20re%20racial%20disparities%20in%20COVID%20response.pdf
- United States Department of Health and Human Services, Task Force on Black and Minority Health. (1985, August). Report of the Secretary’s Task Force on Black and Minority Health. https://collections.nlm.nih.gov/catalog/nlm:nlmuid-8602912-mvset
